Most people assume a lisp is just “cute speech” or lazy tongue work. However, the real reason lies in how breath, tongue shape, and tiny spaces between teeth create (or disrupt) a razor-thin hiss. If the terms sibilance, alveolar ridge, or orofacial myofunctional disorder ring a bell, you’re already close to the answer—just not quite there yet. By the end, the mechanics will make why people have a lisp feel less like a mystery and more like a small mouth-physics lesson.
Voices across time
Early teachers, doctors, and therapists noticed that some speech sounds trip people more than others. Over the last century, they grouped these patterns and wrote about when errors are part of learning and when they persist. Encyclopedias describe lisping as a kind of articulation issue (a problem producing speech sounds)—different from language problems—because it’s mainly about shaping airflow and placement, not vocabulary or grammar.
As clinics grew, specialists also separated speech-sound disorders into two broad categories: making a sound (articulation) and organizing sound patterns (phonology). That split helped explain why one child might distort “s,” while another swaps entire classes of sounds.
What shapes the sound
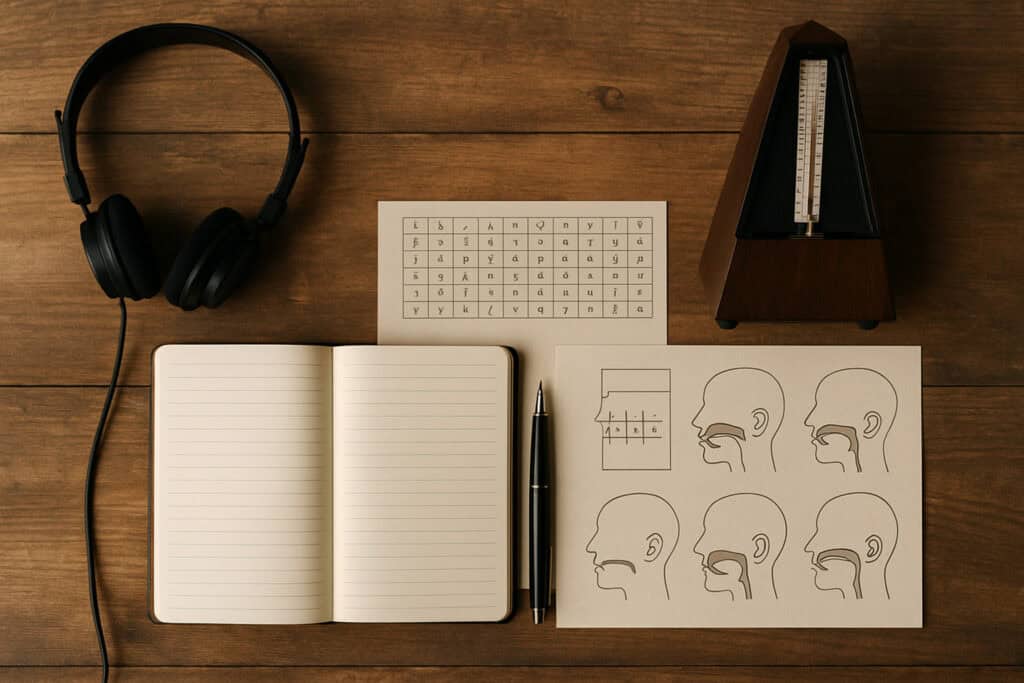
This is where we answer why people have a lisp—by looking at what the breath, tongue, teeth, and brain are actually doing.
The “Central Groove” Physics
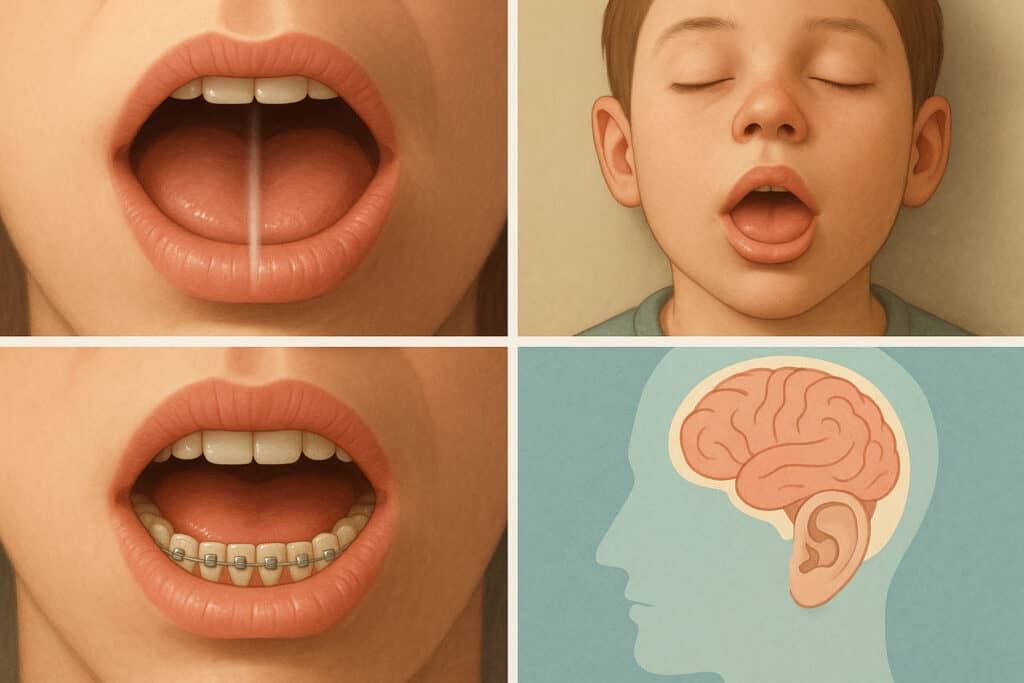
S-sounds are made by pushing air through a narrow channel along the center of the tongue and past the front teeth. When that channel is too wide, too far forward, or pointed sideways, the air scatters. The ear then hears “th” or a “slushy” hiss instead of a crisp “s.” Because that tiny channel is the whole trick, a lisp often shows up when the air doesn’t stay focused down the middle, which is why the sound distorts into a lisp. For general background on how clinicians group these distortions, the Cleveland Clinic explains articulation problems (including lisp-like “s→th” changes) in its guide to articulation disorders.
The “Idle Setting” Problem
Mouths also have “idle settings.” Some people rest with lips apart and the tongue forward; others press the tongue against or between the teeth when swallowing. Over time, that posture can leak into speech and push air the wrong way. Hospitals describe this pattern as tongue thrust (pushing the tongue forward during swallowing or speech), which is part of orofacial myofunctional disorders. Because posture shapes movement, that forward tongue can nudge “s” and “z” into noisy neighbors—and that’s one route to a lisp.
Dental Architecture
Air needs a narrow exit. Gaps from missing teeth, a very open bite, or crowding change the “nozzle.” Even temporary changes—like braces or an aligner—can alter the path of air and where the tongue aims. Because the mouth is a small machine, tiny spacing shifts can bend the sound, so bite or spacing issues can contribute to a lisp until placement is relearned.
Auditory Mapping Errors
Brains build “maps” for sounds by mixing what we feel in the tongue with what we hear. If hearing is muffled early in life (ear infections, for example) or if a person never practiced a clean “s,” the map for that sound may settle in the wrong spot. Because practice sets the default, the mouth repeats the same off movement—so this learned pattern is another reason people keep a lisp. (In speech, a ‘map’ refers to the brain’s pattern for making specific sounds.)
Language transfer and style
Not every “different” s-sound is a disorder. Some languages use a softer or different “s,” and those patterns can transfer when someone speaks English. Also, a few people style their “s” on purpose—for identity or performance. Because those cases follow a plan rather than a problem, they aren’t what clinicians diagnose. In those moments, the sound isn’t a mechanical error; it’s a social choice.
Frequently Asked Questions
“Is every lisp the same?”
Different airflow problems create different results. Air spilling forward can make “s” sound like “th”; air leaking over the sides makes a “wet” hiss. Because the tongue can miss the target in more than one way, clinicians talk about interdental, dentalized, lateral, and palatal variants—so no one label fits all.
“Will kids outgrow it?”
Some patterns fade as coordination improves, especially the mild forward version in very young kids. Because lateral or palatal airflow isn’t part of typical development, those usually stick without targeted practice—which is why a check-in with a speech-language pathologist is recommended when it persists.
“Do braces fix or cause a lisp?”
Changing the bite changes the path of air exit. That shift can briefly blur “s” sounds and also make space for cleaner airflow later. Because teeth and tongue share the job, orthodontics alone isn’t a guarantee, but combined with placement practice, it can help, which is why some people notice improvement after dental work plus therapy.
“Is a lisp a language problem?”
Language is about words and meaning; a lisp is about shaping one sound. Because the issue is mechanical timing and posture, not vocabulary, many people with a lisp speak and understand just fine, so it’s classified with articulation, not language.
“Can adults change it?”
Mouths and brains stay trainable. With feedback (mirrors, recordings), careful placement drills, and sometimes help addressing rest posture, many adults adjust their “s.” Because habit loops are strong, it often takes steady practice, which is why people have a lisp in adulthood, and it often comes down to old motor maps that can still be redrawn.
Bonus: quick, fun facts

Beyond the clinic, the physics of the ‘S’ sound creates a few surprising ripples in music and medicine.
- Recording engineers refer to harsh “s” energy as sibilance and use de-essers to tame it. That studio trick underscores the same physics that drives a lisp: tiny changes in airflow make big changes in sound.
- Some speech clinics coordinate with dentists and ENTs when rest posture, allergies, or nasal airflow affect speech. That team approach is common in pediatric centers like Johns Hopkins All Children’s, where tongue thrust, bite, and speech are evaluated together.
- In population snapshots, speech-sound challenges are common in early grades. That’s a reminder that why people have a lisp isn’t rare or strange—it’s part of how complex speech learning can be in real life.
Final word
Understanding the mouth as a system of valves, grooves, and small tunnels shows that people having a lisp is not a character flaw but a specific airflow issue with multiple causes and solutions. This view encourages curiosity instead of judgment, leading to practical changes. If a single sound can depend on a millimeter of space, consider how small adjustments elsewhere can create meaningful change.
Interested in exploring similar posts? Visit The Science of Everyday Life hub for more!