Hiccups are usually blamed on eating too fast or drinking something fizzy, but, as you will learn today, they actually come from a built-in reflex that links the diaphragm to the throat and the brainstem. Pay careful attention to “phrenic nerve,” “vagus nerve,” “glottis closure,” and “central pattern generator” so you understand how they all work together and what is really going on.
Old cures, new clues

Long before doctors mapped nerves, people tried everything from holding their breath to drinking water upside down. Those tricks spread because hiccups are common and usually pass quickly. Over time, simple descriptions turned into folklore, yet medical writers kept collecting observations. Today, standard references describe hiccups as a brief spasm of the diaphragm followed by a snap shut of the vocal cords that makes the sound we all know, and they list everyday triggers like overeating and stomach distention right alongside medical causes that need attention.
Stories about extreme cases helped too. Charles Osborne reportedly hiccupped for decades, which pushed clinicians to look harder at the brain and nerves involved, not just the stomach. That odd piece of history still shows up in modern summaries and reminds us that while most hiccups are harmless, some point to deeper problems.
Hidden reflex circuitry
The question many people ask is why people get hiccups in the first place. To understand that, start with the wiring rather than the sound.
Afferent alarms
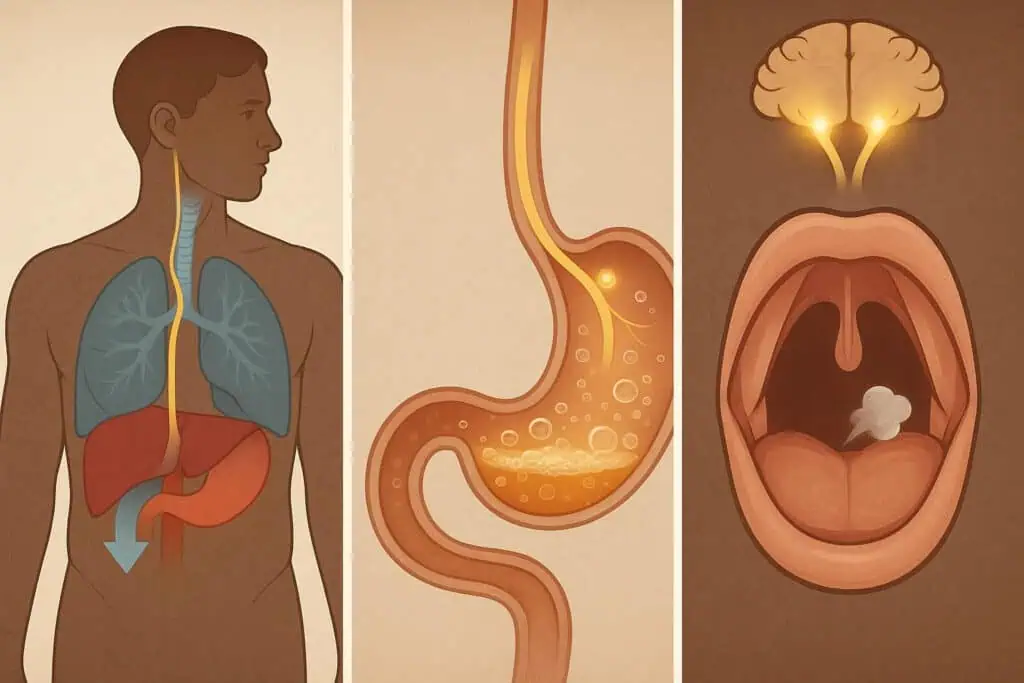
First, the system needs a reason to fire. Stretch sensors in the stomach and esophagus can send signals when you swallow air, overfill the stomach, or drink something very cold or very hot. These messages travel along the vagus nerve and other sensory fibers toward the brainstem. Irritation of the phrenic nerve, which controls the diaphragm, can also set things off. Because these pathways form a “reflex arc,” they can trigger without your conscious control. Clinical explainers from major centers lay out this pathway clearly, noting how vagus and phrenic inputs converge to kickstart an event.
Brainstem timing
Next, a small network in the brainstem acts like a metronome. Researchers often call this a “central pattern generator,” because it can produce rhythmic outputs without conscious control. Neurochemical studies suggest that transmitters like GABA, dopamine, and serotonin help tune that rhythm. When the balance shifts, the pattern generator may misfire and produce rhythmic spasms. That is why some medicines that change these neurotransmitters can either provoke or calm hiccups. A review of the neurochemistry lays out those players and how they relate to the hiccup pattern seen in clinics and labs.
Diaphragm snap and glottis shut
Then, the pulse travels outward through the phrenic nerve, which contracts the diaphragm suddenly. Air rushes toward the lungs, and almost instantly the vocal cords close at the glottis. That closure is why the sound appears. The sequence is tight: a brief inhale, a shut valve, and a tiny pressure pop. Because the steps are locked together, you cannot simply “decide” to stop them once the reflex has started. Nevertheless, controlling breath or swallowing can sometimes interrupt the chain. That is the mechanism behind many home remedies. Only near the end of this cascade can you see the true answer: hiccups are a reflex loop where incoming signals, a brainstem timer, and outgoing motor nerves work in series to create a quick diaphragm spasm and a glottal closure.
Triggers and red flags
Finally, not all hiccups are created equal. Most episodes start with simple triggers, such as overeating, carbonation, temperature swings, or sudden excitement. However, when hiccups last beyond two days, doctors start looking for irritation or injury along the vagus or phrenic nerves, for brain or spinal conditions, for metabolic problems, or for medicine side effects. That is why persistent spells deserve medical attention.
Frequently Asked Questions
Do quick “tricks” actually work?
Many do something useful before they do anything magical. The goal is to reset the reflex, either by changing carbon dioxide levels with a breath hold, by stimulating the vagus nerve with a strong swallow or sip, or by engaging the diaphragm on purpose. A newer device called the Forced Inspiratory Suction and Swallow Tool, often sold as a special straw, tries to combine those actions. In a cross-sectional study, participants reported high rates of relief compared with home remedies, likely because the suction and swallow stimulate both the phrenic and vagus pathways at once. Because it is not a cure-all and the study design has limits, you should still treat it as a tool rather than a guarantee.
Are hiccups only about the stomach?
The stomach is a frequent starting point, yet the wiring runs through the chest and neck to the brainstem, so several body systems can be involved. That is why severe heartburn, ear problems, or even some infections may play a part, and why clinicians check for neurological and metabolic causes when hiccups drag on. Only when symptoms last or come with other warning signs should you shift from home care to medical evaluation.
Which medicines help if hiccups do not stop?
Because the reflex runs on neurotransmitters, some drugs that calm those circuits can help. Doctors sometimes try baclofen, metoclopramide, or, in specific cases, chlorpromazine. These are prescription decisions, so they belong to a clinician after a workup. The key point is the mechanism: by nudging the brainstem timing and the diaphragm output, medicines can make the reflex less likely to fire. Only after trying simple measures and looking for causes should medication enter the plan.
Bonus: Fun Facts

Beyond the obvious triggers, the science of the hiccup reflex suggests a strange evolutionary origin.
A possible evolutionary echo
Scientists have floated a striking idea about the origin of the reflex. In tadpoles, early gill ventilation uses a pattern that looks a lot like a hiccup: an inward draw paired with a closed path that keeps water out of the lungs. Because mammal embryos show hiccup-like patterns early on, some researchers suspect today’s hiccup reflects ancient circuitry that once supported gill-based breathing and later got repurposed for feeding behaviors like suckling. The idea is still a hypothesis, but it neatly fits the wiring and timing.
Why babies hiccup so much
Infants spend a lot of time coordinating breathing and swallowing, and their reflexes are still maturing. Because their stomachs distend easily and their neural timing is still settling, hiccups appear often and usually mean nothing serious. As the nervous system refines those pattern generators, the frequency tends to fall. Parents often ask why babies get hiccups so much in the first months, and the simplest answer is practice: the system is learning to separate breathing, swallowing, and feeding without tripping the reflex.
What your choices change
Your habits can nudge the system toward calm. Eating smaller portions, slowing your pace, avoiding big gulps of carbonation, and keeping alcohol modest reduce the chances of distending the stomach or irritating the esophagus. Because those inputs travel straight into the reflex arc, small changes in behavior often pay off quickly.
Final Word
Seeing hiccups as a reflex rather than a random quirk changes the way you respond. Instead of guessing, you can aim each remedy at a step in the loop, and you can judge when a spell is just a trivial blip versus a nudge to check your health. The next time a “hic” interrupts you, try viewing it as a tiny demonstration of how much your body runs on automatic, and consider how many other everyday mysteries might be hiding the same kind of wiring. If knowing the reason people get hiccups made you look twice at your own habits, what other “small” reflexes deserve a closer look?
Interested in exploring similar posts? Visit The Science of Everyday Life hub for more!